
















Understanding the difference starts with how the models work
In clinical trials, laboratory strategy is not only an operational choice. It directly affects data consistency, interpretation and regulatory acceptance.
Central Lab vs Local Laboratories? In the local laboratory model, each site uses its own laboratory or a nearby provider. This allows for fast turnaround and immediate access to results but introduces variability. Across one study, different laboratories may use different analytical methods, equipment and reference ranges, meaning that the same parameter can be measured differently depending on the location.
This lack of standardization becomes a challenge when data needs to be compared across sites or used for statistical analysis. Additional effort is then required to align results, interpret discrepancies, and ensure consistency.
The central laboratory model addresses this by standardizing testing conditions across the study. Instead of variability being managed later, it is reduced at the source. Read more about Data Harmonization.
When to use each model in practice?
The choice between central and local laboratories depends on what matters most in a given study: consistency or turnaround time.
Central laboratories are the preferred option when data comparability is critical. This applies in multicountry trials, studies with complex biomarkers or endpoints requiring high analytical precision, or custom analytical approach. For example, in oncology trials, centralized biomarker testing is used to ensure that patient stratification is based on consistent and comparable results across all sites.
Local laboratories are more suitable when immediate access to results is required. This includes safety testing, routine assessments or situations where clinical decisions must be made without delay. For example, a patient’s blood count (e.g. white blood cells or platelets) is typically assessed locally to determine whether treatment can be administered on the same day.
In practice, most studies use a combination of both models, often referred to as a hybrid model, where central laboratories handle key endpoints and standardized analyses, while local laboratories support time-critical assessments.
From a cost and operational perspective, the choice often comes down to a trade-off between logistics and data processing effort. Local laboratories may reduce logistics costs but increase the workload for statisticians and programmers who need to align and interpret data from multiple sources. Central laboratories shift this effort upfront into logistics and coordination, but significantly reduce downstream complexity.
Key Takeaways: Central Lab vs Local Laboratories
Choosing central lab vs local laboratories is not about selecting a better model. It is about aligning the laboratory strategy with study requirements.
Local laboratories support speed and immediate decision-making at site level. Central laboratories ensure consistency, data quality and comparability across the study. Using local laboratories where standardization is required increases variability and shifts complexity to the data analysis stage, often requiring additional work to harmonize results.
A central laboratory standardizes processes from the beginning, simplifies data handling, and reduces operational complexity. It also reduces the need for additional coordination on the sponsor side, as one partner manages the full laboratory scope.
While central laboratory models may involve higher logistics costs upfront, they are often more cost-effective in the long term due to reduced effort in data cleaning, harmonization and analysis. This also limits the need for additional internal resources to coordinate multiple laboratory providers.
In most clinical trials, the optimal approach is a structured combination of both models, clearly defining where each should be used.
FAQ: central lab vs local laboratories
1. What is the main difference central lab vs local laboratories in clinical trials?
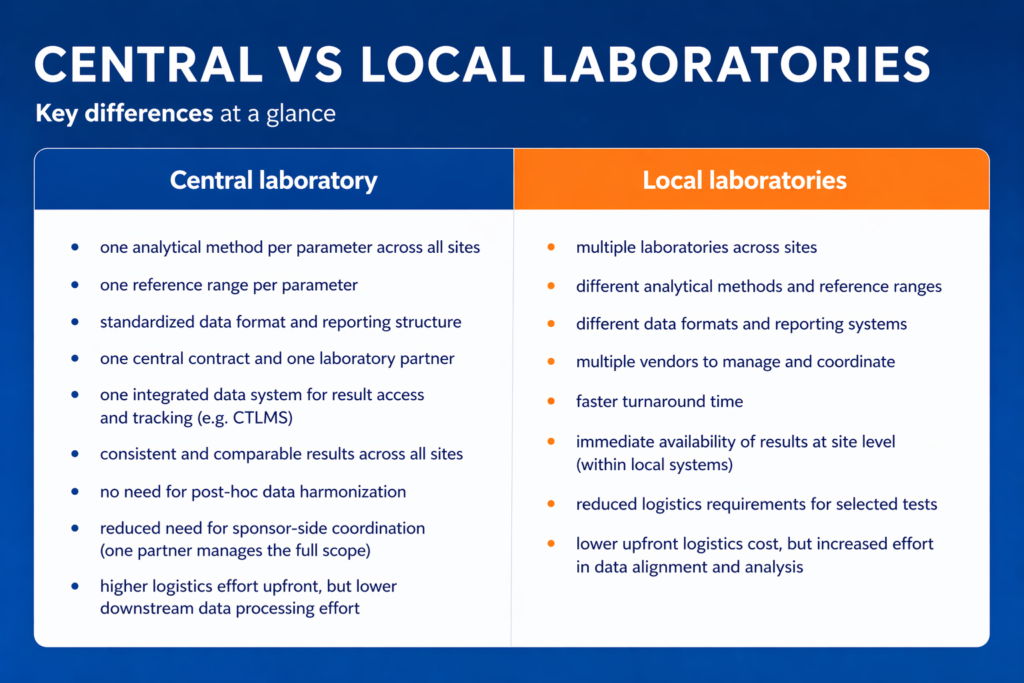
Central laboratories standardize testing across all sites using one method, one reference range, and one data system. Local laboratories operate independently at each site, often using different methods, ranges, and reporting formats, which can introduce variability.
2. When should a central laboratory model be used?
A central laboratory is preferred when data consistency and comparability are critical, such as in multicountry trials, biomarker-driven studies, or trials requiring high analytical precision and standardized endpoints.
3. When are local laboratories more appropriate?
Local laboratories are suitable when rapid turnaround is essential, particularly for safety testing or routine assessments where immediate clinical decisions must be made at the site level.
4. What are the main operational trade-offs between central lab vs local laboratories?
Central laboratories require more upfront logistics and coordination but reduce downstream data processing and harmonization efforts. Local laboratories offer faster access to results but increase the complexity of data alignment and analysis later in the study.
5. Is it possible to combine central lab and local laboratory models in one study?
Yes, most clinical trials use a hybrid model. Central laboratories handle key endpoints and standardized analyses, while local laboratories support time-critical tests, allowing both consistency and speed where needed.
References (supporting)
- Central vs Local Labs – Clinical Research Made Simple, clinicalstudies.in, access date 24.04.2026
- Conducting Clinical Trials With Decentralized Elements | FDA, FDA, access date: 23.04.2026
- Choosing Different Labs Based on the Therapeutic Area of a Study | Applied Clinical Trials Online, Applied Clinical Trials, access date: 23.04.2026